Welcome to
American Eagle Medical




Welcome to
American Eagle Medical
Welcome to American Eagle Medical, the creators and exclusive source of Pi’s Pillow, the revolutionary new solution to positioning patients for ventilation and intubation.
The Pi’s Pillow is made of high quality foam and consists of two parts, a base and a removable pad (figure 1). The pillow has both disposable and reusable models (figure 2). The disposable pillow is in a vacuum package and can be easily stored within a small operating room of a hospital. The reusable pillow is good for limiting waste and is economical for a hospital’s budget. The pillow is available in four sizes: small, medium, large and extra-large. The small size is for smaller, pediatric patients; and the extra-large Pi's Pillow or Pi's Obesity Pillow is extremely useful when treating obese patients.

Pi's Pillow consists of a removable and adjustable pad/head-piece (on top) and a base (on bottom).

Reusable pi’s Pillow (regular size).

Before intubation, operator uses his right hand to push patient's head forward and in extension.
The Head Position for Endotracheal Intubation and the Pi’s Pillow
Appropriate positioning of the patient is paramount to successful mask ventilation. With the patient in the supine position, the head and neck are placed in the sniffing position (1). Successful direct laryngoscopy for exposure of the glottis opening requires alignment of the oral, pharyngeal, and laryngeal axes (2). Elevation of the head, slight flexion of the neck on the thorax and severe extension of the head on the neck at the atlanto-occipital joint, accomplishes the best possible alignment of the oral, pharyngeal, and laryngeal axes. This posture is described as the “sniff position” (3, 4). This position maximally opens the airway, moves the epiglottis out of the visual line, and maximally reduces airway resistance (4). The extension of the atlanto-occipital point also provides anterior displacement of the mass of the tongue and an advantage in mouth opening (5).
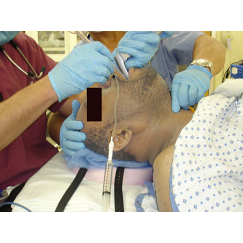
There is no support cushion available in the clinical setting to keep a patient’s head in the extension position. To maintain the desired axis the laryngoscopist has to use the laryngoscope blade to lift the patient’s chin up by his or her left hand to maintain the patient’s head in the extension position, and at the same time, use his or her right hand to advance the endotracheal tube into the laryngeal inlet and trachea. Here is a very skillful operator gently and carefully performing intubation (figure 3 & 4). In a teaching hospital, very often, an anesthesiologist assists the resident by holding a patient’s head in the extension position (figure 5).

During intubation, head extension is maintained by the laryngocsope, the operator's left hand, and his right wrist and palm.
A resident is intubating with head positioning help.
Pi's Pillow is comfortable for an awake patient.
Using a laryngoscope blade to keep the patient’s head in the extension position, places enormous weight on the blade, even for a patient who is of average size. It is the upper front teeth, pharyngeal and laryngeal tissue that receive the most pressure from the blade. Lifting a patient’s chin up forcefully by a laryngoscope blade may cause dental, pharyngeal and laryngeal tissue damage. Very often patients complain of pharyngeal and laryngeal pain after intubation. Also, the position created by the laryngoscope is not stable and any little movement may ruin a good view because there is an empty space beneath the lower head and upper neck. If the head extension position is unable to be achieved by lifting a patient’s chin to visualize the glottis opening, repeated or traumatic tracheal intubation attempts may occur and could cause more severe complications such as vocal cord avulsion, recurrent nerve damage, hematoma or laryngeal spasm and upper airway edema.
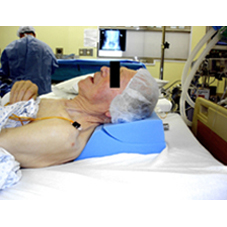
Thus, Pi’s Pillow (figure 1) has been developed to support the patient’s head in full extension position and maintain proper alignment of the three axes of the upper airway, whenever the intubation is performed. As per the book of Clinical Anesthesia: “A Pi’s Pillow which is comfortable for the awake patient, but easily reconfigured after anesthetic induction to provide an ideal position has been developed by Dr. Kaiduan Pi”.

After induction the pad is removed and a patient is ventilated.

The base of Pi's Pillow creates an ideal position for an intubation.

The base of the pillow creates an ideal position for LMA insertion.
The pillow not only maximizes the airway opening to facilitate mask ventilation and intubation, but also significantly decreases the chances of damaging the patient’s teeth and tissue around the airway during intubation because there is no struggle with the intubation. Main Point: Maintaining the head in extension during intubation can be accomplished using Pi’s Pillow instead of using the laryngoscope, thus, reducing the chance of damaging airway tissue. Since the laryngeal inlet is already visible by using the pillow, lifting the chin up forcefully by using the laryngoscope is unnecessary. Also, the pillow helps manage a difficult airway because the position maintained by the pillow is so stable. The good view or spot will not be lost. Pi’s Pillow makes ventilation and intubation by one person easy, safe and efficient (figure 6, 7, 8 & 9).
Reference:
1. Barash PG, Cullen BF, Stoelting RK: Clinical Anesthesia, p 600, Philadelphia, Lippincott Williams & Wilkins, 2006
2. Miller RD: Miller’s Anesthesia, p1622, Philadelphia, Elsevier Churchill Livingstone, 2005
3. Miller RD: Miller’s Anesthesia, p1633, Philadelphia, Elsevier Churchill Livingstone, 2005
4. Barash PG, Cullen BF, Stoelting RK: Clinical Anesthesia, pp 606-607, Philadelphia, Lippincott Williams & Wilkins, 2001
5. Barash PG, Cullen BF, Stoelting RK: Clinical Anesthesia, pp 609-610, Philadelphia, Lippincott Williams & Wilkins, 2006